Thanks to a dedicated and supportive community, SARRC has spent over two decades advancing the understanding and treatment of autism. But what did the autism landscape look like back in 1997? We asked members of SARRC’s research team to reflect on those early days. Here’s a glimpse of how far we’ve come since then.
What is the prevalence of autism among children in the United States?
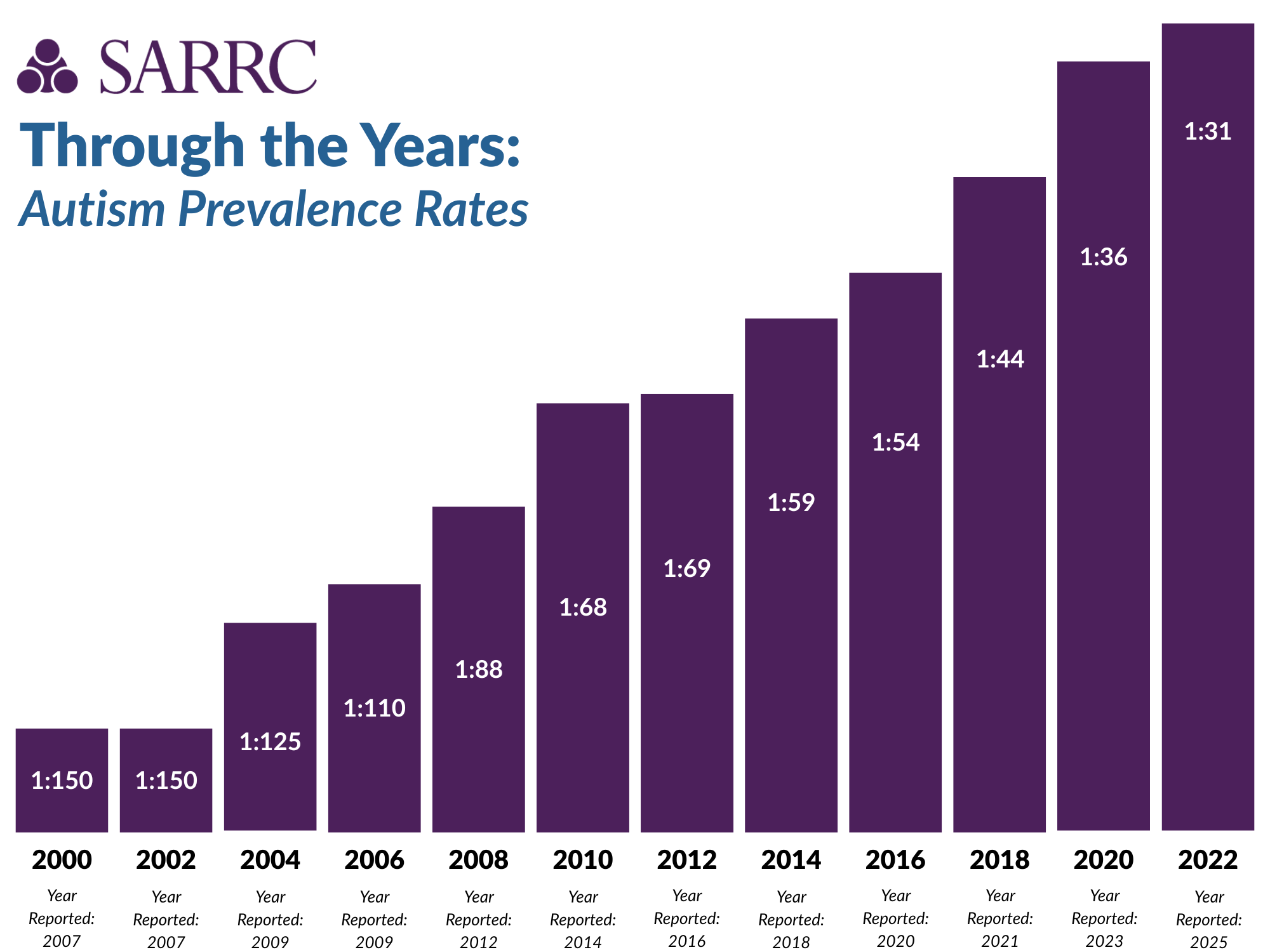
In 1997, autism was on the rise, and so were people’s concerns, yet there were no dedicated efforts to monitor prevalence rates. In 1995, rough estimates suggested that 1 in 500 children were likely to be diagnosed with autism. In the year 2000, the Centers for Disease Control and Prevention (CDC) began carefully tracking prevalence rates through the Autism and Developmental Disabilities Monitoring Network. Today, the CDC reports that 1 in 31 children has been identified with autism spectrum disorder (ASD).
What is the average age children are receiving an autism diagnosis?
The estimated average age of diagnosis in the U.S. was 4 years, 4 months in 1997. While parental concerns were noted in earlier development, it was more common for children to be identified and diagnosed upon reaching school age. As of 2025, the CDC reports that the average age of diagnosis in the U.S. is 3 years, 11 months. However, research has shown that a reliable diagnosis of autism can be made as early as 2 years old.
What does the existing body of scientific research say about what factors are driving rising autism rates?
One of the most significant shifts occurred in 2013 with the release of the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders), the diagnostic manual used by professionals to identify mental and developmental conditions. This revision consolidated several previously separate diagnoses, such as autistic disorder, Asperger’s disorder, and Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS) — into a single diagnosis: autism spectrum disorder (ASD). This broadened the diagnostic criteria, resulting in more individuals falling under the ASD umbrella compared to the earlier DSM-IV framework.
At the same time, growing public awareness, evolving treatment approaches, and increased visibility of children with autism in public education settings have all contributed to higher recognition and diagnosis rates. As people become more familiar with the signs of autism, it’s more likely that individuals who may have been missed in the past are now being identified.
When looking at reported prevalence over time, earlier estimates have increased, but recent data from the CDC have shown a relatively stable pattern, hovering around 1 in 44, 1 in 36, and 1 in 31 in the last few reports. These smaller incremental changes, as opposed to sharp spikes in increases, suggest the effect of the diagnostic changes is leveling off, and we’re approaching a more accurate and consistent understanding of autism prevalence in the general population.
What does existing research say about what causes autism?
There’s no solid scientific evidence that points to a single cause for autism. Instead, research shows that autism is a complex condition with many different contributing factors.
These can range from genetic influences to environmental ones — or most likely, a mix of both. In fact, scientists have found links between autism and hundreds of different genes, which underscores just how multifaceted it is.
Autism isn’t something that can be “cured,” but it is best considered an alternate developmental pathway, where some are much more profoundly impaired than others. Autism is not a disease, so there is no cure. Instead, the best strategy is intervention that helps autistic individuals learn and develop skills that lead to their personal, optimal level of independence.
Is there any research into whether environmental factors are linked to rising autism rates?
Scientists have explored a variety of environmental toxins, none of which have been firmly implicated as a clearly linked cause that explains all — or even a significant minority — of why people have autism. There have been many changes in our environment over the past three decades that may be correlated with the rising rates of autism, from air pollution and rising carbon dioxide in our atmosphere to the use of technology and cell phones. But as we were all taught in basic high school science, correlation does not imply causation. Forgetting that basic tenet of science can lead to a significant waste of precious resources that could be better directed toward more legitimate scientific endeavors.
What are the expected outcomes for adults with autism?
When SARRC was founded in 1997, very little was known about the outcomes for adults with autism. The prevalence of autism was continually increasing, but long-term expectations were unclear. While many large care facilities closed in the 1980s, it was not uncommon for institutionalization to be suggested as part of the care of people with autism. Children who were diagnosed in 1997 are young adults now, and places like SARRC are working to build and shape inclusive employment and educational opportunities. According to a 2017 National Autism Indicators Report, only 14 percent of adults with autism had a job for pay outside of the home within the first two years after leaving high school. Over the next decade, it is estimated that up to 1 million youth with autism will transition to adulthood and may be seeking employment.
What factors, if any, influence how often boys vs. girls are diagnosed with autism?
Studies consistently find higher rates of autism in boys than girls. Currently, the male-to-female ratio for autism is estimated to be 3:1. This gender gap is narrowing (it used to be 4:1 or even slightly larger), and improvements in identifying autism in girls have led to research aiming to understand the disparity and to determine whether or not girls are being underdiagnosed. While the results are not yet definitive, the body of research that is starting to emerge is promising for early diagnosis in females, and that is invaluable. However, the gender gap is still prominent, which implicates genetics as the most likely cause of autism.
Early research on autism planted a seed for a male stereotype of the disorder and led to diagnostic procedures being largely male-biased, using male norms. In reality, females often present differently. They may have fewer repetitive behaviors, and their restricted interests may be more socially acceptable and therefore go unnoticed. They may also have a more socially appropriate communication style. With these social camouflaging traits, females are more likely to appear as if they are fitting in when they’re young, so it doesn’t raise a flag.
Common stereotypes and gendered expectations about females in general may help fuel the possibility of underdiagnosing girls. Females with autism often demonstrate some appropriate social skills. They may have good eye contact, develop language and gestures on time, and demonstrate social motivation, which can be misleading to parents and pediatricians. However, they may show subtle social differences, like making odd or too many social initiations, misreading social cues, and engaging in repetitive speech.
How have diagnostic criteria changed in the past 20 years?
Autistic disorder, Asperger’s disorder, and Pervasive Developmental Disorder (PDD) were three distinct developmental disorders with different diagnostic criteria, namely a lack of significant language delay in individuals with Asperger’s and an atypical onset or atypical presentation of autism associated with PDD. The division between these three developmental disorders often causes issues related to access to services as well as general care.
In 2013, the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) newly identified autism as autism spectrum disorder (ASD), folding all subcategories of the condition into one umbrella diagnosis. Autistic disorder, Asperger’s disorder, and PDD are no longer considered separate conditions.
Since our founding, SARRC has remained dedicated to conducting innovative research, providing evidence-based practices, disseminating effective training, and building inclusive communities for individuals with autism and their families.
Learn more about early intervention services at SARRC
Diagnostic Services »
Do you suspect autism or have concerns about your child’s development?
Easy Access Autism Screening »
If you have concerns about your child’s development and want answers fast, access a free developmental screening with our team.
Milestones »
A free program offering information on developmental milestones for parents of infants ages 6 to 18 months.
Free Online Family Orientation »
Monthly meetings that connect parents to current information and resources related to ASD.
Updated May 2025